




Minimizing Consequences of Complex Interventions

Dr. Darren B. Schneider
Under the leadership of Darren B. Schneider, MD, Chief of Vascular and Endovascular Surgery, NewYork-Presbyterian/ Weill Cornell Medical Center is offering Investigational Device Exemptions to study branched and fenestrated stent-graft devices for the treatment of complex thoracoabdominal aortic aneurysms (TAAA). Two years ago, the participating centers formed the United States Aortic Research Consortium to pool their data on patients who have received the devices. “The consortium now has combined data on over 1,000 patients,” notes Dr. Schneider. “Our goal is to establish a web-based central data coordinating center that will help facilitate group research projects, taking this nationwide collaborative research to the next level.”
At the Eastern Vascular Society annual meeting in September 2019, Dr. Schneider and his Weill Cornell colleagues presented their work in employing near-infrared spectroscopy to monitor the collateral circulation to the spinal cord during endovascular repair of TAAA. “The experience from three centers using this technique in over 100 patients showed that it was more specific than other monitoring techniques and may be more clinically beneficial guiding these procedures,” says Dr. Schneider. “We also use this monitoring to dictate whether it’s safe to complete the entire repair or leave some blood flow into the aorta and aneurysm and then return on another day to complete the repair. Since starting this protocol, we’ve had no cases of paraplegia in 50 consecutive patients.”
The Weill Cornell physicians will soon launch a study to monitor the recovery of patients who have had minimally invasive branched and fenestrated TAAA repairs. “Patients wear fitness trackers so that we can remotely monitor their activity level and heart rate to detect any problem,” says Dr. Schneider.
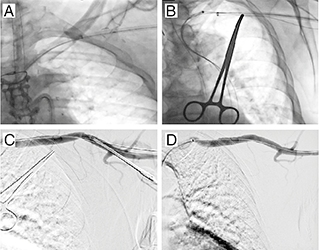
Safe closure of a percutaneous axillary artery access site involves (A) a 90 cm long femoral artery sheath intussuscepted into the end of the axillary artery sheath and advanced into the distal subclavian artery (B) advancing the safety wire from the femoral sheath across the axillary artery puncture site into the brachial artery (C) removal of axillary artery sheath leaving Glidewire in place (D) completion angiogram following removal of axillary artery Glidewire
In a study published online in the August 2019 issue of the Annals of Vascular Surgery, Weill Cornell’s vascular surgeons demonstrated the safety and efficacy of percutaneous axillary artery access in patients requiring upper extremity large sheath access during complex aortic interventions. “We can perform these repairs via a percutaneous approach with zero incisions — just a puncture through the skin to enter the artery at the top of each leg and a small puncture near the left shoulder to enter the axillary artery,” explains Dr. Schneider. “Operative times and wound-related complications may be reduced and the procedure is very easy to tolerate.”
Dr. Schneider and his team also have developed a minimally invasive technique for transcarotid artery revascularization by directly accessing the carotid artery through a keyhole incision at the base of the neck. “We can create a shunt and reverse flow in the artery to prevent particles from breaking off and traveling to the brain.”
The Weill Cornell surgeons also use advanced 3-D image fusion technology for its potential to reduce IV contrast volume, radiation exposure, and procedure and fluoroscopy time. Construction of a new state-of-the-art hybrid operating suite with fusion imaging guidance and next generation imaging equipment is currently underway.