




General Information About Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer
This PDQ summary addresses the staging and treatment of ovarian epithelial cancer, fallopian tube cancer (FTC), and primary peritoneal cancer (PPC).
Regardless of the site of origin, the hallmark of these cancers is their early peritoneal spread of metastases. The inclusion of FTC and PPC within the ovarian epithelial cancer designation is generally accepted because of much evidence that points to a common Müllerian epithelium derivation and similar management of these three neoplasms. The hypothesis that many high-grade serous ovarian cancers (the most common histological subtype) may arise from precursor lesions that originate in the fimbriae of the fallopian tubes has been supported by findings from risk-reducing surgeries in healthy women with BRCA1 or BRCA2 variants.[1] In addition, histologically similar cancers diagnosed as primary peritoneal carcinomas share molecular findings, such as loss or inactivation of the tumor-suppressor p53 and BRCA1 or BRCA2 proteins.[2] Therefore, high-grade serous adenocarcinomas arising from the fallopian tube and elsewhere in the peritoneal cavity, together with most ovarian epithelial cancers, represent extrauterine adenocarcinomas of Müllerian epithelial origin and are staged and treated similarly to ovarian cancer. Since 2000, FTC and PPC have usually been included in ovarian cancer clinical trials.[3]
Clear cell and endometrioid ovarian cancers that are linked to endometriosis have different gene-expression signatures, as do mucinous subtypes.[2]
Stromal and germ cell tumors are relatively uncommon and comprise fewer than 10% of cases. For more information, see Ovarian Germ Cell Tumors Treatment and Ovarian Borderline Tumors Treatment.
Incidence and Mortality
Epithelial carcinoma of the ovary is one of the most common gynecologic malignancies, with almost 50% of all cases occurring in women older than 65 years. It is the sixth most frequent cause of cancer death in women.[4,5]
Estimated new cases and deaths from ovarian cancer in the United States in 2025:[5]
- New cases: 20,890.
- Deaths: 12,730.
Anatomy
The fimbriated ends of the fallopian tubes are in close apposition to the ovaries and in the peritoneal space, as opposed to the corpus uteri (body of the uterus) that is located under a layer of peritoneum.
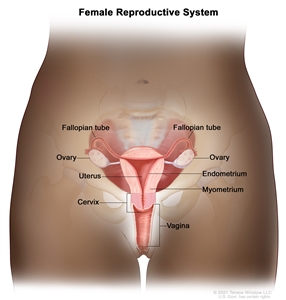
Normal female reproductive system anatomy.
Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for ovarian (epithelial) cancer include:
- Family history of ovarian cancer.[6,7,8]
- A first-degree relative (e.g., mother, daughter, or sister) with the disease.
- Inherited risk.[9]
- Other hereditary conditions such as hereditary nonpolyposis colorectal cancer (HNPCC; also called Lynch syndrome).[6,9]
- Endometriosis.[11,12,13]
- Hormone therapy.[14,15]
- Postmenopausal hormone replacement therapy.
- Obesity.[16,17,18]
- High body mass index.
- Tall height.[16,17,18]
Family history and genetic alterations
The most important risk factor for ovarian cancer is a history of ovarian cancer in a first-degree relative (mother, daughter, or sister). Approximately 20% of ovarian cancers are familial, and although most of these are linked to pathogenic variants in either the BRCA1 or BRCA2 gene, several other genes have been implicated.[19,20] The risk is highest in women who have two or more first-degree relatives with ovarian cancer.[21] The risk is somewhat less for women who have one first-degree relative and one second-degree relative (grandmother or aunt) with ovarian cancer.
In most families affected with breast and ovarian cancer syndrome or site-specific ovarian cancer, genetic linkage to the BRCA1 locus on chromosome 17q21 has been identified.[22,23,24]BRCA2, also responsible for some instances of inherited ovarian and breast cancer, has been mapped by genetic linkage to chromosome 13q12.[25]
The lifetime risk of developing ovarian cancer in patients with germline pathogenic variants in BRCA1 is substantially increased over that of the general population.[26,27] Two retrospective studies of patients with germline pathogenic variants in BRCA1 suggest that the women in these studies have improved survival compared with those without BRCA1 variants.[28,29][Level of evidence C1] Most women with BRCA1 variants probably have family members with a history of ovarian and/or breast cancer. Therefore, the women in these studies may have been more vigilant and inclined to participate in cancer screening programs that may have led to earlier detection.
For women at increased risk, prophylactic oophorectomy may be considered after age 35 years if childbearing is complete. A family-based study included 551 women with BRCA1 or BRCA2 variants. Of the 259 women who had undergone bilateral prophylactic oophorectomy, 2 (0.8%) developed subsequent papillary serous peritoneal carcinoma, and 6 (2.8%) had stage I ovarian cancer at the time of surgery. Of the 292 matched controls, 20% who did not have prophylactic surgery developed ovarian cancer. Prophylactic surgery was associated with a reduction in the risk of ovarian cancer that exceeded 90% (relative risk, 0.04; 95% confidence interval, 0.01–0.16), with an average follow-up of 9 years.[30] However, family-based studies may be associated with biases resulting from case selection and other factors that influence the estimate of benefit.[31] After a prophylactic oophorectomy, a small percentage of women may develop a PPC that is similar in appearance to ovarian cancer.[32] This risk of developing PPC is likely related to the presence of serous tubal intraepithelial carcinoma (STIC) at the time of prophylactic oophorectomy. In a large study that pooled patients with BRCA variants from several sources, women with a STIC lesion were nearly 34 times more likely to develop PPC than women without such a lesion. This finding highlights the need for accurate and thorough pathological review of the prophylactic oophorectomy specimen to help with individual patient counseling.[33]
For more information, see Ovarian, Fallopian Tube, and Primary Peritoneal Cancers Prevention and BRCA1 and BRCA2: Cancer Risks and Management.
Clinical Presentation
Ovarian epithelial cancer, FTC, or PPC may not cause early signs or symptoms. When signs or symptoms do appear, cancer is often advanced. Signs and symptoms include:
- Pain, swelling, or a feeling of pressure in the abdomen or pelvis.
- Urinary urgency or frequency.
- Difficulty eating or feeling full.
- A lump in the pelvic area.
- Gastrointestinal problems such as gas, bloating, or constipation.
These symptoms often go unrecognized, leading to delays in diagnosis. Efforts have been made to enhance physician and patient awareness of the occurrence of these nonspecific symptoms.[34,35,36,37,38]
Screening procedures such as gynecologic assessment, vaginal ultrasonography, and cancer antigen 125 (CA-125) assay have had low predictive value in detecting ovarian cancer in women without special risk factors.[39,40] As a result of these confounding factors, annual mortality in ovarian cancer is approximately 65% of the incidence rate.
Most patients with ovarian cancer have widespread disease at presentation. Early peritoneal spread of the most common subtype of high-grade serous cancers may relate to serous cancers starting in the fimbriae of the fallopian tubes or in the peritoneum, readily explaining why such cancers are detected at an advanced stage. Conversely, high-grade serous cancers are underrepresented among stage I cancers of the ovary. Other types of ovarian cancers are, in fact, overrepresented in cancers detected in stages I and II. This type of ovarian cancer usually spreads via local shedding into the peritoneal cavity followed by implantation on the peritoneum and via local invasion of bowel and bladder. The incidence of positive nodes at primary surgery has been reported to be as high as 24% in patients with stage I disease, 50% in patients with stage II disease, 74% in patients with stage III disease, and 73% in patients with stage IV disease. The pelvic nodes were involved as often as the para-aortic nodes.[41] Tumor cells may also block diaphragmatic lymphatics. The resulting impairment of lymphatic drainage of the peritoneum is thought to play a role in development of ascites in ovarian cancer. Transdiaphragmatic spread to the pleura is common.
Diagnostic and Staging Evaluation
The following tests and procedures may be used in the diagnosis and staging of ovarian epithelial cancer, FTC, or PPC:
- Physical examination and history.
- Pelvic examination.
- CA-125 assay.
- Ultrasonography (pelvic or transvaginal).
- Computed tomography (CT) scan.
- Positron emission tomography (PET) scan.
- Magnetic resonance imaging (MRI).
- Chest x-ray.
- Biopsy.
CA-125 levels can be elevated in other malignancies and benign gynecologic problems such as endometriosis. CA-125 levels and histology are used to diagnose epithelial ovarian cancer.[42,43]
Prognostic Factors
Prognosis for patients with ovarian cancer is influenced by multiple factors. Multivariate analyses suggest that the most important favorable prognostic factors include:[44,45,46,47,48]
- Younger age.
- Good performance status.
- Cell type other than mucinous or clear cell.
- Well-differentiated tumor.
- Early-stage disease.
- Absence of ascites.
- Lower disease volume before surgical debulking.
- Smaller residual tumor after primary cytoreductive surgery.
- BRCA1 or BRCA2 variant.
For patients with stage I disease, the most important prognostic factor associated with relapse is grade, followed by dense adherence and large-volume ascites.[49] Stage I tumors have a high proportion of low-grade serous cancers. These cancers have a derivation distinctly different from that of high-grade serous cancers, which usually present in stages III and IV. Many high-grade serous cancers originate in the fallopian tube and other areas of extrauterine Müllerian epithelial origin.
If the tumor is grade 3, densely adherent, or stage IC, the chance of relapse and death from ovarian cancer is as much as 30%.[49,50,51,52]
The use of DNA flow cytometric analysis of tumors from patients with stage I and stage IIA disease may identify those at high risk.[53] Patients with clear cell histology appear to have a worse prognosis.[54] Patients with a significant component of transitional cell carcinoma appear to have a better prognosis.[55]
Case-control studies suggest that women with BRCA1 and BRCA2 variants have improved responses to chemotherapy when compared with patients with sporadic epithelial ovarian cancer. This may be the result of a deficient homologous DNA repair mechanism in these tumors, which leads to increased sensitivity to chemotherapy agents.[56,57]
Follow-Up After Treatment
Because of the low specificity and sensitivity of the CA-125 assay, serial CA-125 monitoring of patients undergoing treatment for recurrence may be useful. However, whether that confers a net benefit has not yet been determined. There is little guidance about patient follow-up after initial induction therapy. Neither early detection by imaging nor by CA-125 elevation has been shown to alter outcomes.[58] For more information, see the Treatment of Recurrent or Persistent Ovarian Epithelial, Fallopian Tube, and Primary Peritoneal Cancer section.
References:
- Levanon K, Crum C, Drapkin R: New insights into the pathogenesis of serous ovarian cancer and its clinical impact. J Clin Oncol 26 (32): 5284-93, 2008.
- Birrer MJ: The origin of ovarian cancer—is it getting clearer? N Engl J Med 363 (16): 1574-5, 2010.
- Dubeau L, Drapkin R: Coming into focus: the nonovarian origins of ovarian cancer. Ann Oncol 24 (Suppl 8): viii28-viii35, 2013.
- National Cancer Institute: SEER Stat Fact Sheets: Ovarian Cancer. Bethesda, Md: National Institutes of Health. Available online. Last accessed February 10, 2025.
- American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025. Available online. Last accessed January 16, 2025.
- Bolton KL, Ganda C, Berchuck A, et al.: Role of common genetic variants in ovarian cancer susceptibility and outcome: progress to date from the Ovarian Cancer Association Consortium (OCAC). J Intern Med 271 (4): 366-78, 2012.
- Weissman SM, Weiss SM, Newlin AC: Genetic testing by cancer site: ovary. Cancer J 18 (4): 320-7, 2012 Jul-Aug.
- Hunn J, Rodriguez GC: Ovarian cancer: etiology, risk factors, and epidemiology. Clin Obstet Gynecol 55 (1): 3-23, 2012.
- Pal T, Akbari MR, Sun P, et al.: Frequency of mutations in mismatch repair genes in a population-based study of women with ovarian cancer. Br J Cancer 107 (10): 1783-90, 2012.
- Gayther SA, Pharoah PD: The inherited genetics of ovarian and endometrial cancer. Curr Opin Genet Dev 20 (3): 231-8, 2010.
- Poole EM, Lin WT, Kvaskoff M, et al.: Endometriosis and risk of ovarian and endometrial cancers in a large prospective cohort of U.S. nurses. Cancer Causes Control 28 (5): 437-445, 2017.
- Pearce CL, Templeman C, Rossing MA, et al.: Association between endometriosis and risk of histological subtypes of ovarian cancer: a pooled analysis of case-control studies. Lancet Oncol 13 (4): 385-94, 2012.
- Mogensen JB, Kjær SK, Mellemkjær L, et al.: Endometriosis and risks for ovarian, endometrial and breast cancers: A nationwide cohort study. Gynecol Oncol 143 (1): 87-92, 2016.
- Lacey JV, Brinton LA, Leitzmann MF, et al.: Menopausal hormone therapy and ovarian cancer risk in the National Institutes of Health-AARP Diet and Health Study Cohort. J Natl Cancer Inst 98 (19): 1397-405, 2006.
- Trabert B, Wentzensen N, Yang HP, et al.: Ovarian cancer and menopausal hormone therapy in the NIH-AARP diet and health study. Br J Cancer 107 (7): 1181-7, 2012.
- Engeland A, Tretli S, Bjørge T: Height, body mass index, and ovarian cancer: a follow-up of 1.1 million Norwegian women. J Natl Cancer Inst 95 (16): 1244-8, 2003.
- Lahmann PH, Cust AE, Friedenreich CM, et al.: Anthropometric measures and epithelial ovarian cancer risk in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer 126 (10): 2404-15, 2010.
- Collaborative Group on Epidemiological Studies of Ovarian Cancer: Ovarian cancer and body size: individual participant meta-analysis including 25,157 women with ovarian cancer from 47 epidemiological studies. PLoS Med 9 (4): e1001200, 2012.
- Lynch HT, Watson P, Lynch JF, et al.: Hereditary ovarian cancer. Heterogeneity in age at onset. Cancer 71 (2 Suppl): 573-81, 1993.
- Pennington KP, Swisher EM: Hereditary ovarian cancer: beyond the usual suspects. Gynecol Oncol 124 (2): 347-53, 2012.
- Piver MS, Goldberg JM, Tsukada Y, et al.: Characteristics of familial ovarian cancer: a report of the first 1,000 families in the Gilda Radner Familial Ovarian Cancer Registry. Eur J Gynaecol Oncol 17 (3): 169-76, 1996.
- Miki Y, Swensen J, Shattuck-Eidens D, et al.: A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 266 (5182): 66-71, 1994.
- Easton DF, Bishop DT, Ford D, et al.: Genetic linkage analysis in familial breast and ovarian cancer: results from 214 families. The Breast Cancer Linkage Consortium. Am J Hum Genet 52 (4): 678-701, 1993.
- Steichen-Gersdorf E, Gallion HH, Ford D, et al.: Familial site-specific ovarian cancer is linked to BRCA1 on 17q12-21. Am J Hum Genet 55 (5): 870-5, 1994.
- Wooster R, Neuhausen SL, Mangion J, et al.: Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science 265 (5181): 2088-90, 1994.
- Easton DF, Ford D, Bishop DT: Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am J Hum Genet 56 (1): 265-71, 1995.
- Struewing JP, Hartge P, Wacholder S, et al.: The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med 336 (20): 1401-8, 1997.
- Rubin SC, Benjamin I, Behbakht K, et al.: Clinical and pathological features of ovarian cancer in women with germ-line mutations of BRCA1. N Engl J Med 335 (19): 1413-6, 1996.
- Aida H, Takakuwa K, Nagata H, et al.: Clinical features of ovarian cancer in Japanese women with germ-line mutations of BRCA1. Clin Cancer Res 4 (1): 235-40, 1998.
- Rebbeck TR, Lynch HT, Neuhausen SL, et al.: Prophylactic oophorectomy in carriers of BRCA1 or BRCA2 mutations. N Engl J Med 346 (21): 1616-22, 2002.
- Klaren HM, van't Veer LJ, van Leeuwen FE, et al.: Potential for bias in studies on efficacy of prophylactic surgery for BRCA1 and BRCA2 mutation. J Natl Cancer Inst 95 (13): 941-7, 2003.
- Piver MS, Jishi MF, Tsukada Y, et al.: Primary peritoneal carcinoma after prophylactic oophorectomy in women with a family history of ovarian cancer. A report of the Gilda Radner Familial Ovarian Cancer Registry. Cancer 71 (9): 2751-5, 1993.
- Steenbeek MP, van Bommel MHD, Bulten J, et al.: Risk of Peritoneal Carcinomatosis After Risk-Reducing Salpingo-Oophorectomy: A Systematic Review and Individual Patient Data Meta-Analysis. J Clin Oncol 40 (17): 1879-1891, 2022.
- Goff BA, Mandel L, Muntz HG, et al.: Ovarian carcinoma diagnosis. Cancer 89 (10): 2068-75, 2000.
- Friedman GD, Skilling JS, Udaltsova NV, et al.: Early symptoms of ovarian cancer: a case-control study without recall bias. Fam Pract 22 (5): 548-53, 2005.
- Smith LH, Morris CR, Yasmeen S, et al.: Ovarian cancer: can we make the clinical diagnosis earlier? Cancer 104 (7): 1398-407, 2005.
- Goff BA, Mandel LS, Melancon CH, et al.: Frequency of symptoms of ovarian cancer in women presenting to primary care clinics. JAMA 291 (22): 2705-12, 2004.
- Goff BA, Mandel LS, Drescher CW, et al.: Development of an ovarian cancer symptom index: possibilities for earlier detection. Cancer 109 (2): 221-7, 2007.
- Partridge E, Kreimer AR, Greenlee RT, et al.: Results from four rounds of ovarian cancer screening in a randomized trial. Obstet Gynecol 113 (4): 775-82, 2009.
- van Nagell JR, Miller RW, DeSimone CP, et al.: Long-term survival of women with epithelial ovarian cancer detected by ultrasonographic screening. Obstet Gynecol 118 (6): 1212-21, 2011.
- Burghardt E, Girardi F, Lahousen M, et al.: Patterns of pelvic and paraaortic lymph node involvement in ovarian cancer. Gynecol Oncol 40 (2): 103-6, 1991.
- Berek JS, Knapp RC, Malkasian GD, et al.: CA 125 serum levels correlated with second-look operations among ovarian cancer patients. Obstet Gynecol 67 (5): 685-9, 1986.
- Atack DB, Nisker JA, Allen HH, et al.: CA 125 surveillance and second-look laparotomy in ovarian carcinoma. Am J Obstet Gynecol 154 (2): 287-9, 1986.
- Omura GA, Brady MF, Homesley HD, et al.: Long-term follow-up and prognostic factor analysis in advanced ovarian carcinoma: the Gynecologic Oncology Group experience. J Clin Oncol 9 (7): 1138-50, 1991.
- van Houwelingen JC, ten Bokkel Huinink WW, van der Burg ME, et al.: Predictability of the survival of patients with advanced ovarian cancer. J Clin Oncol 7 (6): 769-73, 1989.
- Neijt JP, ten Bokkel Huinink WW, van der Burg ME, et al.: Long-term survival in ovarian cancer. Mature data from The Netherlands Joint Study Group for Ovarian Cancer. Eur J Cancer 27 (11): 1367-72, 1991.
- Hoskins WJ, Bundy BN, Thigpen JT, et al.: The influence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 47 (2): 159-66, 1992.
- Thigpen T, Brady MF, Omura GA, et al.: Age as a prognostic factor in ovarian carcinoma. The Gynecologic Oncology Group experience. Cancer 71 (2 Suppl): 606-14, 1993.
- Dembo AJ, Davy M, Stenwig AE, et al.: Prognostic factors in patients with stage I epithelial ovarian cancer. Obstet Gynecol 75 (2): 263-73, 1990.
- Ahmed FY, Wiltshaw E, A'Hern RP, et al.: Natural history and prognosis of untreated stage I epithelial ovarian carcinoma. J Clin Oncol 14 (11): 2968-75, 1996.
- Monga M, Carmichael JA, Shelley WE, et al.: Surgery without adjuvant chemotherapy for early epithelial ovarian carcinoma after comprehensive surgical staging. Gynecol Oncol 43 (3): 195-7, 1991.
- Kolomainen DF, A'Hern R, Coxon FY, et al.: Can patients with relapsed, previously untreated, stage I epithelial ovarian cancer be successfully treated with salvage therapy? J Clin Oncol 21 (16): 3113-8, 2003.
- Schueler JA, Cornelisse CJ, Hermans J, et al.: Prognostic factors in well-differentiated early-stage epithelial ovarian cancer. Cancer 71 (3): 787-95, 1993.
- Young RC, Walton LA, Ellenberg SS, et al.: Adjuvant therapy in stage I and stage II epithelial ovarian cancer. Results of two prospective randomized trials. N Engl J Med 322 (15): 1021-7, 1990.
- Gershenson DM, Silva EG, Mitchell MF, et al.: Transitional cell carcinoma of the ovary: a matched control study of advanced-stage patients treated with cisplatin-based chemotherapy. Am J Obstet Gynecol 168 (4): 1178-85; discussion 1185-7, 1993.
- Vencken PM, Kriege M, Hoogwerf D, et al.: Chemosensitivity and outcome of BRCA1- and BRCA2-associated ovarian cancer patients after first-line chemotherapy compared with sporadic ovarian cancer patients. Ann Oncol 22 (6): 1346-52, 2011.
- Safra T, Borgato L, Nicoletto MO, et al.: BRCA mutation status and determinant of outcome in women with recurrent epithelial ovarian cancer treated with pegylated liposomal doxorubicin. Mol Cancer Ther 10 (10): 2000-7, 2011.
- Rustin GJ, van der Burg ME, Griffin CL, et al.: Early versus delayed treatment of relapsed ovarian cancer (MRC OV05/EORTC 55955): a randomised trial. Lancet 376 (9747): 1155-63, 2010.